This is a research paper I wrote about the choice to provide treatment to an extremely premature infant. I wrote about how that choice is made and how it should be made. I analyzed several papers and studies about extreme prematurity and concluded that the decision should be individually made for each infant and should be based on multiple factors.
There has long been a debate about how doctors should decide whether or not to treat infants born at the borderline of viability (the stage at which a fetus gains the ability to survive outside the womb). The focus of much of this debate has been on gestational age and finding a certain number of weeks before which infants should not receive treatment and after which they should. There are, however, several other factors besides gestational age at birth that affect an infant’s chances of survival and chances of having disabilities if they do survive. These factors include the infant’s birthweight, sex, whether the fetus is a singleton or one of a multiple birth, and whether the infant received prenatal steroids to improve their lung development (Brunkhorst et al.). In fact, a study done in 2008 by the National Institute of Child Health and Human Development (NICHD) showed that these four characteristics were able to give a more accurate prediction of an infant’s outcome than gestational age alone (Brunkhorst et al.). This shows that it is important to consider many aspects of a fetus or infant’s situation when making the decision to either commence or withhold treatment. This paper offers an opinion on how to make that decision without only taking into account gestational age at birth.
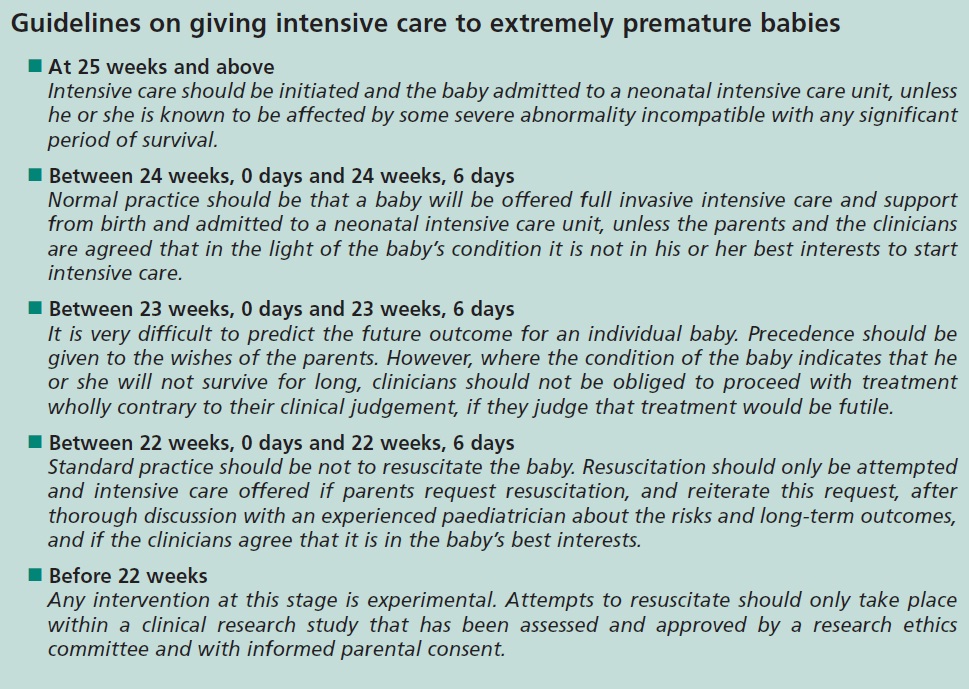
The Nuffield Council on Bioethics, in the U.K., has issued guidelines for the decision of whether to treat extremely premature infants, shown here below. The Council recommends that before 22 weeks, an infant should not be resuscitated except as part of a research study because it would be considered “an experimental procedure” (Chiswick). Between 22 and 23 weeks, resuscitation is not recommended. Between 23 and 24 weeks, the Council leaves the decision of whether to treat the infant largely up to the parents. Between 24 and 25 weeks, the Council recommends resuscitation unless the infant’s parents and doctors agree that it would not be “in his or her best interests” (Nuffield). At and after 25 weeks, infants should always be resuscitated unless they have a “severe abnormality incompatible with any significant period of survival” (Nuffield). There at least seems to be general agreement within the neonatology community about the upper and lower thresholds of borderline viability (that infants born before 22 weeks should not be resuscitated, and those born at or after 25 weeks should almost always be resuscitated), although some, like the majority of the clinicians at a consensus conference in New South Wales, might disagree with the Nuffield Council’s recommendations for each week in between. The Nuffield Council guidelines for infants born at 23 weeks whose parents have not had the chance to discuss their options are that treatment should be given to the infant until the parents are given the information they need to make a decision. The overwhelming majority of participants in the New South Wales Conference, more than 90%, would not resuscitate an infant born at 23 weeks if the parents could not or would not make a decision about treatment.

{kind=link}
I believe that the Nuffield Council’s guidelines should be taken into consideration along with the other factors mentioned above when deciding whether to attempt treatment. If an infant is born at a very early gestational age but is larger than average for their gestational age, has been treated with prenatal steroids, et cetera, their gestational age should not prevent them from receiving treatment if there are other indications of a good outcome.
The National Institute of Child Health and Human Development has an online calculator that shows the survival rate of an infant depending on gestational age, birthweight, sex, singleton versus multiple pregnancy, and whether the fetus was treated with steroids. A 22-week male fetus in a multiple pregnancy that weighs 430 grams and had not received prenatal steroids would have a 6% chance of survival if mechanically ventilated, according to the NICHD’s online calculator, whereas a 22-week female fetus in a singleton pregnancy that weighs 625 grams and did receive prenatal steroids would have a 39% chance of survival if treated with mechanical ventilation. She would still be more likely to die than survive, but her chance of survival is 6.5 times higher than the other fetus even though they are at the same gestational age. This shows how important it is to not make decisions based solely on the infant’s gestational age.
It is true that as an infant’s gestational age at birth increases, their risk of mortality and serious early morbidity decreases. For example, one study found that infants born before 24 weeks gestation had a 67% chance of having a disability at one year old, whereas infants born at 24 weeks or later had a 13% chance of disability (Ahner et al.). This study also found that an infant’s chance of survival if born at 24 weeks is 50% (Ahner et al.). The likelihood of an infant to survive without disabilities reaches 50% at 25 weeks gestation. However, gestational age is not the only factor correlated with the rates of survival and disability. This is also true of birthweight: with increasing birthweight, there is decreasing risk of mortality and morbidity (Ahner et al.). Thus birthweight should also be taken into consideration. An unusually high birthweight might give an infant better chances than an average infant at the same gestational age.
Some studies have found that survival rates of infants born at a certain gestational age have improved over time. The lowest gestational age and birthweight at which it is possible for an infant to survive was previously considered to be 28 weeks and 1000 grams (Eidelman). Ever since the 1960s, the gestational age at which it is possible for an infant to survive has decreased by about one week every ten years (Kuschel and Kent). A study conducted in Chicago showed that by 2008, the mortality rate for infants born before 26 weeks had decreased to 28%, from 80% in 1988 (Gillam et al.). A U.K. study found that the survival rate for infants born between 24 and 26 weeks increased from 1996 to 2003 (Chiswick). These results would suggest that outcomes are continually improving for extremely premature infants. One might use this data to argue for a policy of resuscitation, attesting that improvements in medicine and neonatology will result in more infants surviving if treated.
However, other studies have not shown a reduced mortality rate over time, or have provided evidence that this improvement does not extend to infants born at the earliest limits of viability. The same study from the U.K. also found that the survival rate for infants born at 23 weeks had not increased from 1996 to 2003 (Chiswick). There is also the issue of morbidity (disease) aside from mortality (death). A 2006 study called EPICure 2 compared its results to its earlier counterpart, EPICure, which used data from infants born in 1995, and found that while the survival rate for infants born at 24-25 weeks had increased during that time, rates of early morbidity for the same gestational age had remained similar (Kuschel and Kent). As shown in the figure below, the survival rate for all gestational age weeks in the EPICure studies increased from 1995 to 2006, although some of the increase might be attributed to the fact that the survival rate from 1995 reflects the percentage of all infants who survived, while the 2006 survival rate only measures the percentage of treated infants who survived. The largest increases in survival rate were at the higher gestational age weeks, and there was only a tiny increase in the survival rate for infants born at 22 weeks. This data might support the claim that only infants born after a certain gestational age should be resuscitated and treated, maybe 23 weeks and later, since the survival rate for 22-week infants remains almost the same and still very low after 11 years.

There is an assumption that parents will not have to be responsible for deciding whether to have their infant treated because they will, at birth, show signs of either a good or poor prognosis. Actually, the condition of an infant at birth does not necessarily indicate a certain outcome. For example, an infant’s Apgar score does not accurately predict long- or even short-term outcome (Chiswick). It is not a good indicator of mortality past the first 24 hours of life (Kuschel and Kent). One study additionally revealed that clinicians could not predict better than chance whether an infant lived or died based on how the infant presented at birth (Kuschel and Kent). This contradicts the assumption that an infant’s outcome can be known or predicted accurately at birth. In fact, “physiologic response” in the early days of life cannot predict many conditions, including bronchopulmonary dysplasia, iatrogenic infection, necrotizing enterocolitis, patent ductus arteriosus, and retinopathy of prematurity (Leuthner). However, there are some early indicators that can predict a higher chance of mortality before discharge from NICU (neonatal intensive care unit), such as a heart rate lower than 100 beats per minute at 5 minutes old and a body temperature less than 35 degrees Celsius (95 degrees Fahrenheit) when admitted to NICU (Leuthner). Still, an infant should not be denied treatment based on their presentation at birth if they would statistically have a good chance of a positive outcome.
In the United States the Emergency Medical Treatment and & Labor Act, or EMTALA, does not mandate resuscitation for infants born at borderline viability, but does claim that there should be a screening examination of the infant (Leuthner). Some have argued that the birth of an extremely premature infant should be considered an emergency, which would make itunnecessary to receive informed consent from the parents before resuscitating and treating their child. This claim of emergency would also mandate a “trial of assessment and treatment” for the infant (Leuthner). The claim has four premises:
(1) assessment of gestational age after birth is more accurate; (2) assessment of vigorousness adds prognostic information; (3) testing treatment responses in first hours to days provides more facts or certainty to help determine long-term prognosis and therefore decreases speculation; and (4) treatment withdrawal is ethically equivalent to withholding, from the parents’ perspective. (Leuthner).
Leuthner goes on to say that if all four of these premises are not true, mandated assessment and treatment are not justified. It could be argued that, in fact, none of these premises are true. Methods of determining gestational age in utero might actually be more accurate than the methods used postnatally (Leuthner). With Apgar scores as a measure of vigorousness, it has been shown above that there is no correlation with prognosis. Also mentioned above is the evidence that the infant’s condition in early days does not predict long-term outcome. Lastly, although withdrawing treatment is legally equivalent to withholding treatment, some parents and doctors are more reluctant to decide to stop treatment once it has been started than to decide from birth not to treat. Leuthner argues that since there is evidence showing that the premises of this emergency argument are false, treatment should not be mandatory.
One factor that is very important in making the decision of whether to treat is the survival rate for infants at a certain gestational age. However, statistics of survival rates for extremely premature infants might be misleading. The figure above showing results from the EPICure studies is an example of this, as is data from The National Institute of Child Health and Human Development. The NICHD data showed a 6% survival rate for infants born at 22 weeks gestation (Brunkhorst et al.). Only 13% of infants in this study who were born at 22 weeks received steroids in utero that would help their lung development, and only 19% were intubated and treated with mechanical ventilation (Brunkhorst et al.). Thus, the 6% survival rate might have been different if all infants in the study had been given steroids prenatally and treated postnatally (an infant born at 22 weeks might actually have a chance of survival greater than 6% if they are actually treated). This is evidenced by reported survival rates in different countries. A 2009 study published by the Japan Pediatric Society found the survival rate for infants born at 22 weeks to be 34%, and for infants born at 24 weeks 77%, which are much higher rates than other studies have reported (Brunkhorst et al.). It is routine in Japan to resuscitate and treat infants born as early as 22 to 23 weeks gestation, which could explain their higher chances of survival. In Switzerland, where there are guidelines against resuscitating extremely premature infants, their survival rate is 4%. The survival rate of Swiss infants born at 24 and 25 weeks is higher, but not as high as the survival rate for infants born at the same gestation in other countries (Brunkhorst et al.).
Clinicians should not have a gestational age cut-off or birthweight cut-off for treatment, such as 24 weeks or 500 grams. They should also not decline to treat an infant just because of a low Apgar score, or another observation from the infant’s very early days of life, if the parents want their child to be treated. The decision-making should mostly be left to the parents, unless the doctors believe the infant has no chance of survival, in which case they would not treat even if the parents wished for treatment, or a good enough chance that parental wishes of no resuscitation should be overridden. No one characteristic should disqualify an infant from being treated.
WORKS CITED
Ahner, Regine, et al. “Ethical Implications of Aggressive Obstetric Management at Less than 28 Weeks of Gestation.” Acta Obstetricia Et Gynecologica Scandinavica, vol. 80, no. 2, 2001, pp. 120–125.
Eidelman, Arthur I. “Dilemmas in the Treatment of Premature Infants at the Borderline of Viability.” Rambam Maimonides Medical Journal, vol. 2, no. 4, 2011, p. e0066.
Brunkhorst, et al. “Infants of Borderline Viability: The Ethics of Delivery Room Care.” Seminars in Fetal and Neonatal Medicine, vol. 19, no. 5, 2014, pp. 290–295.
Chiswick, Malcolm. “Infants of Borderline Viability: Ethical and Clinical Considerations.” Seminars in Fetal and Neonatal Medicine, vol. 13, no. 1, 2008, pp. 8–15.
French, Noel. “Consensus Statement on Perinatal Care.” Journal of Paediatrics and Child Health, vol. 43, no. 6, 2007, pp. 492–493.
Gillam, Lynn, et al. “Decision‐Making at the Borderline of Viability: Who Should Decide and on What Basis?” Journal of Paediatrics and Child Health, vol. 53, no. 2, 2017, pp. 105–111.
“Guidelines on Intensive Care for Extremely Premature Babies.” Nuffield Council on Bioethics, Nuffield Council on Bioethics, nuffieldbioethics.org/report/neonatal-medicine-2/guidelines-intensive-care-extremely-premature-babies.
Kuschel, Carl A., and Alison Kent. “Improved Neonatal Survival and Outcomes at Borderline Viability Brings Increasing Ethical Dilemmas.” Journal of Paediatrics and Child Health, vol. 47, no. 9, 2011, pp. 585–589.
Leuthner, Steven R. “Borderline Viability: Controversies in Caring for the Extremely Premature Infant.” Clinics in Perinatology, vol. 41, no. 4, 2014, pp. 799–814.
“NICHD Neonatal Research Network (NRN): Extremely Preterm Birth Outcome Data.” Eunice Kennedy Shriver National Institute of Child Health and Human Development, US Department of Health and Human Services, www1.nichd.nih.gov/epbo-calculator/Pages/epbo_case.aspx.
“Survival.” EPICure, www.epicure.ac.uk/overview/survival/.